
Endovascular management of vascular access is an exciting field that emerged as a valid option for hemodialysis patients extending from stenosis treatment, decloting salvage procedures, hemodialysis catheter insertion, and lately to percutaneous arteriovenous fistula creation. To date, it is considered the gold standard for most of these procedures compared to surgery. To that end, it is an extremely useful service provided to the hemodialysis patient and an important practice field for the interventional radiologist.
by Panagiotis Kitrou MD, MSc, PhD, EBIR, FCIRSE
Associate Professor in Interventional Radiology
Director of the EVA (EndoVascular Access) Meeting
Patras University Hospital, Greece
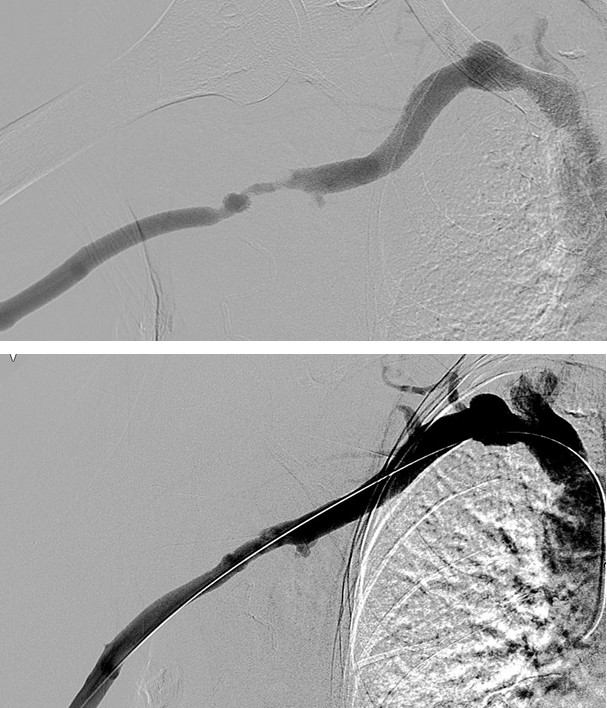
A vascular access is created by anastomosing an artery with a vein and is cannulated with two needles, three times a week for four hours for a patient to receive hemodialysis. Being an artificially created circuit, it will teleologically dysfunction with the main reasons being vessel stenosis within the circuit and thrombosis. Unlike other vascular beds, vascular access is characterized by venous neointimal hyperplasia owed to the proliferation of contractile smooth muscle cells and myofibroblasts, which together with the extracellular matrix produced will create an aggressive fibromuscular thickening. To that end, vascular access stenosis rates are higher compared to peripheral arterial disease, coronary or even carotid disease.
In the past 15 years, endovascular procedures have offered improved outcomes in vascular access treatment. The use of high-pressure balloons, paclitaxel-coated balloons, covered stents and to some extent cutting balloons, significantly improved not only lesion patency but also circuit survival. Devices are nowadays of adequate diameter to cover lesion treatment even at the level of the central thoracic veins. Endovascular decloting procedures cover a broad spectrum of options between thrombectomy and thrombolysis and new dedicated thrombectomy devices offer not only thrombus dissolution but also removal. Both angioplasty procedures for stenosis treatment and decloting procedures are fast procedures with high success rates and are day-cases allowing the patient to immediately return to dialysis without the need of placing a central venous catheter.
In the last 7 years, the percutaneous arteriovenous fistula creation is offered as an additional/supplementary option to surgical creation. The procedures are performed under local anesthesia or nerve block with similar, in most of the cases, results to surgical creation and do not exclude future surgical operation. The reason for this is that the anastomosis is created with the use of the deep venous network of the forearm and blood is drained via the perforator vein at the level of the elbow to the superficial venous network.
Endovascular dialysis access management is an important pathway ranging from creation to maintenance and restoration, offering interventional radiologists an important service and hemodialysis
patients a valid option for improved care and quality of life.


Write a comment